Tennis & Golfers Elbow – Elbow Tendinopathy
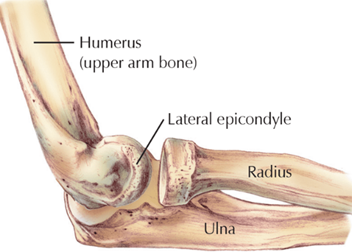
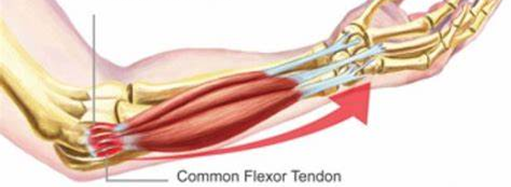
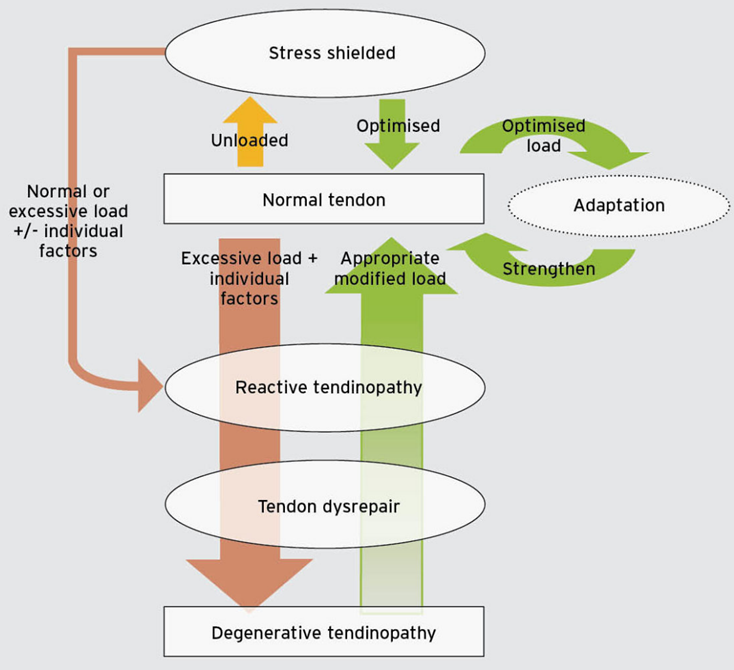
The elbow consists of 3 bones (humerus, radius and ulna) that connect together to form a hinge joint which allows flexion and extension of the arm. Tendinopathies of the elbow typically occur at the attachment points of either the Common Extensor Tendon (the lateral epicondyle) or the Common Flexor Tendon (the medial epicondyle). Epicondyles are the bony ridges situated on either side of the elbow and are the attachment points of various muscles in the forearm which control movements at the wrist. To understand why tendinopathies develop, it’s important to understand the concepts of load and capacity. Capacity refers to the tendons ability to withstand load. When appropriate progressive loads are placed through tendons, the tendons respond beneficially, and tendon strength and integrity improve. However, when the load placed on the tendon exceeds its capacity, injuries will occur. Capacity can be exceeded by either a single load that is too great for the tendon to cope with, or by a cumulative load that overtime exceeds the tendons’ ability to recover and repair itself.
Tennis Elbow (Tendinopathy of the CET):
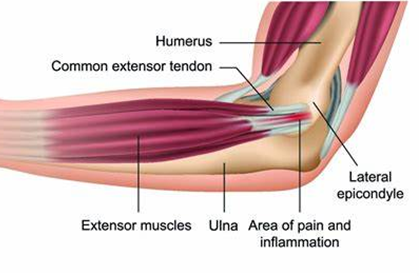
Tennis elbow is a condition where pain is felt on the outside of the elbow, localised to the lateral epicondyle. Pain will gradually increase in intensity overtime and will be worse during activities which involve gripping and extension of the wrist e.g., turning a door handle. The pain is caused by the gradual degeneration of the common extensor tendon (CET) due to repetitive overload of the forearm muscles which use this tendon. The ECRB (Extensor Carpi Radialis Brevis) muscle which controls wrist extension (with forearm pronated) is most likely to become problematic, however, Extensor Digitorum (controls finger extension) and Extensor Carpi Ulnaris (controls wrist extension and adduction) may also be involved.
The tendinopathy can develop for various reasons such as overuse, poor gripping technique, and frequent carrying of heavy loads, especially when carried with a small grip. These factors accumulate and result in an excessive load being applied to the CET which weakens the tendon. If the CET continues to be used whilst in this weakened state, small tears will begin to appear within the tendon and pain will gradually increase.
Despite the name, tennis elbow is more common in those who carry out of manual labour and DIY work due to the requirement for repetitive twisting movements of the forearm and wrist (e.g., when using a screwdriver). The most typical presentation of tennis elbow is an insidious pain which occurs 24-72 hours after unaccustomed activity involving wrist extension e.g., after spending the weekend putting up new furniture. However, pain can also occur immediately after a single instance of exertion e.g., lifting a very heavy object.
In those who do play tennis, this condition may occur due to the use of new equipment e.g., using a new racquet that is too heavy or requires a smaller grip. But it may also be caused by poor technique in which backhand shots are performed with an overreliance on forearm strength with little contribution from the trunk or legs to generate force.
Golfers Elbow (Tendinopathy of the CFT):
Golfer’s elbow is a similar condition but pain is felt on the inside of the elbow and is localised to the medial epicondyle, worsening during activities which involve gripping and/or flexion of the wrist. In this condition, pain develops for similar reasons (repetitive overload of the forearm muscles) but results in the gradual degeneration of the Common Flexor Tendon (CFT). This occurs because repetitive wrist flexion (such as when gripping a golf club) stresses the CFT and overtime this can cause the tendon to become worn down.
It’s also important to know that like Tennis Elbow, many cases of golfer’s elbow may not be sport related and could be due to a person’s occupation. People who work in manual labour or at a desk may be at risk due to the repetitive gripping and/or flexion of the wrist required in their daily lives which leads to the development of the overuse injury.
However, in those who do play golf, the condition may occur due to a suboptimal grip and golf swing technique which forces additional load to go through the wrist flexors during the downswing, impact and release phases.
Management of Golfers Elbow – Similarly to Tennis Elbow, the focus of treatment will be on addressing grip strength and wrist stabilisation as well as on improving load distribution throughout the wrist, forearm and the rest of the body. This will be achieved by progressive optimal loading of the wrist, but will target the CFT through isometrics followed by eccentric wrist flexion exercises. Golf players should also aim to correct any suboptimal techniques which may be resulting in the development of Golfer’s Elbow. E.g., excessive wrist flexion on impact may be occurring due to weakness in the core and legs and will result in reduced stability and the inability to generate sufficient power through weight transfer and hip rotation. By strengthening the muscles which control rotation through the hip and stabilisation of the body, we can ensure appropriate weight transfer from back foot to front foot with effective and coordinated hip rotation.