Common Shoulder Injuries
The shoulder has the greatest available range of motion of any joint within the body, however, this characteristic means the shoulder can be less stable which can result in an increased risk of injury. This post provides a brief overview of the anatomy of the shoulder and details common injuries which may occur. So, if you’re suffering from shoulder pain or instability and want a better understanding of what’s going on, this post is for you!
Anatomy:
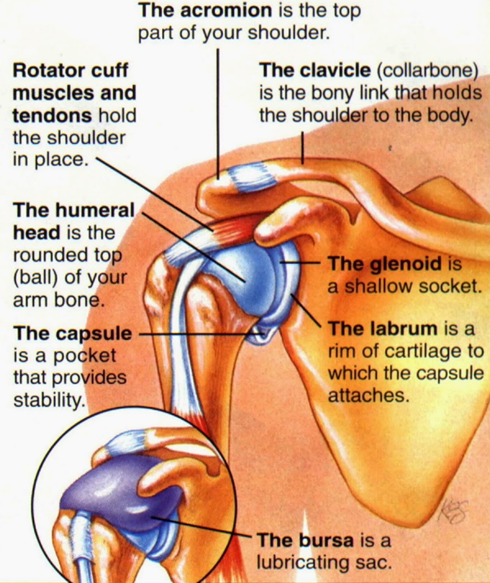
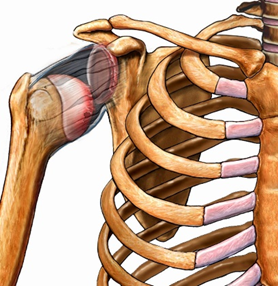
The shoulder (glenohumeral) joint is made up of 2 main bones: the humerus (upper arm) and the scapula (shoulder blade). The head of the humerus is ball shaped and fits into the glenoid cavity (a socket on the scapula). Surrounding the shoulder are various muscles, tendons and ligaments which help to support the shoulder and prevent instability.
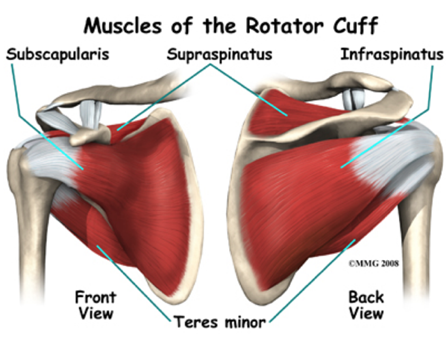
A key muscle group surrounding the shoulder joint is the rotator cuff. This consists of 4 muscles (supraspinatus, infraspinatus, teres minor, subscapularis) which attach in the shoulder to provide stability by ensuring the humeral head is held securely in its socket. An injury to these muscles or their tendons can cause severe pain within the shoulder, and weakness of the rotator cuff can result in various shoulder injuries such as impingement or dislocations.
Common Injuries:
Rotator Cuff Strains/Tears:
Strains (partial rupture) or tears (complete rupture) of the rotator cuff occur due to an inability of the muscle to withstand the load/force being applied to it, e.g., when trying to lift a heavy load with an extended arm. This injury is most commonly seen in older adults whose tendons are already weakened making them more susceptible to further injury. Symptoms will include shoulder pain during activity, especially when lifting the arm overhead, and an inability to sleep on the affected side. Those with more serious injuries will have significant weakness and will be unable to raise the affected arm at all.
Key management/treatment – optimise tissue healing followed by restoration of full function via progressive strengthening exercises.
Rotator Cuff Tendinopathy:
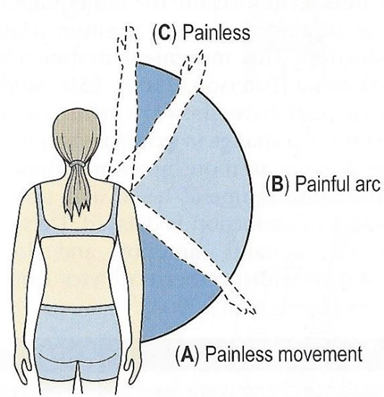
Rotator Cuff Tendinopathy is the degeneration of one or more of the rotator cuff tendons. This typically occurs due to chronic overuse of the rotator cuff muscles and is most commonly seen in active people who undertake lots of overhead movements e.g., tennis players or swimmers. Symptoms include shoulder pain with overhead movements (e.g., throwing a ball) and many clients with this injury will display a painful arc pattern.
Key management/treatment – prevent further irritation of the tendon followed by progressive optimal loading and strengthening of the tendons via eccentric activities.
Long Head of Biceps (LHOB) Tendinopathy:
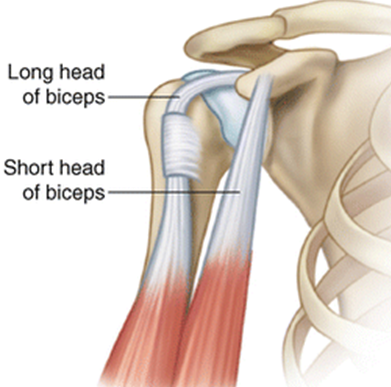
The long head of the biceps tendon attaches within the shoulder and acts as an additional stabiliser of the joint. This tendon can become overloaded due to suboptimal shoulder positioning (shoulders rounded forwards) which causes the biceps to work harder to stabilise the shoulder and overtime will lead to aggravation and inflammation of the LHOB. Symptoms include anterior shoulder pain whilst raising the arm to the front and during a variety of gym exercises (e.g., bench press and bicep curl).
Key management/treatment – preventing further irritation of the tendon followed by rotator cuff strengthening to help draw the shoulders back and down, reducing the load placed on the LHOB when stabilising the shoulder.
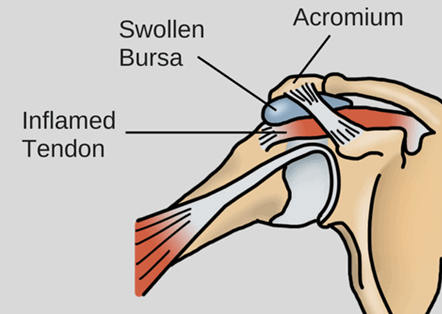
Subacromial Pain Syndromes (SAPS) aka Shoulder Impingement:
One of the most frequently described shoulder conditions that can be a cause or a result of shoulder tendinopathies. This injury is typically caused by repetitive overload of the shoulder which results in inflammation and swelling of tendons/bursa within the subacromial space but can also be associated with suboptimal thoracic posture and/or scapular rhythm. Symptoms will be similar to those found in shoulder tendinopathies dependent on which structures are being impinged and many clients will feel short sharp pain when carrying out everyday activities such as putting on a jacket, combing their hair or reaching into their back trouser jacket.
Key management/treatment – address areas of weakness (e.g., rotator cuffs) and improve stability of the shoulder whilst improving mobility through the thoracic spine. May also need to address the biomechanics of the scapular by optimising movement patterns about the shoulder.
Glenohumeral Instability / Shoulder Dislocation:
Shoulder dislocations can be either traumatic or atraumatic. Traumatic dislocations typically occur in athletes who play contact sports but may also be a result of a fall or collision. 97% of these are anterior dislocations where the head of the humerus is forced out of the socket due to the arm going into excessive abduction and external rotation e.g. when falling onto an outstretched arm. Conversely, atraumatic dislocations are typically a result of multidirectional instability due to hypermobility of the shoulder joint. Symptoms will typically include feeling the joint coming out of place, feelings of shoulder instability and intense pain at time of injury.
Key management/treatment – In most cases where an athlete wants to return to full sport, surgery is recommended followed by intense physiotherapy to restore range of motion and strength within the shoulder. However, dislocations can also be managed conservatively with a focus on strengthening the muscles which stabilise the shoulder to prevent excess movement and reduce the risk of reinjury. Additionally, we can work to enhance your scapular rhythm/movement which can help to relieve symptoms and promote optimal muscle activation, improving stability of the shoulder.
Summary:
Shoulder pain can be complex and may also be referred from the neck, back or spine – so if you have a new or ongoing shoulder issue be sure to book an appointment with Reboot Injury Clinic so we can accurately diagnose you and get you started on a bespoke rehabilitation plan!
Return to blog